The discovery of the Tubarial Gland
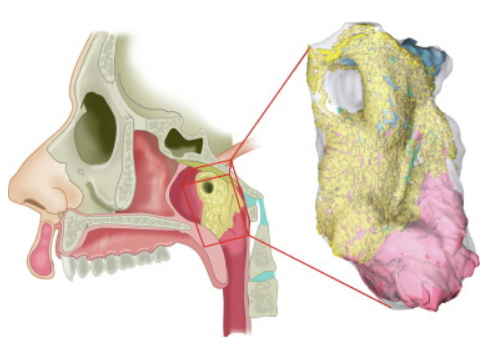
The presence of previously unnoticed bilateral macroscopic salivary gland locations in the human nasopharynx was suspected after visualization by positron emission tomography/computed tomography with prostate-specific membrane antigen ligands (PSMA PET/CT). We aimed to elucidate the characteristics of this unknown entity and its potential clinical implications for radiotherapy.
The human body contains a pair of previously overlooked and clinically relevant macroscopic salivary gland locations, for which we propose the name tubarial glands. Sparing these glands in patients receiving RT may provide an opportunity to improve their quality of life.
Link to Tubareal Gland papers: Pubmed
Studying surgical anatomy using micro-CT imaging
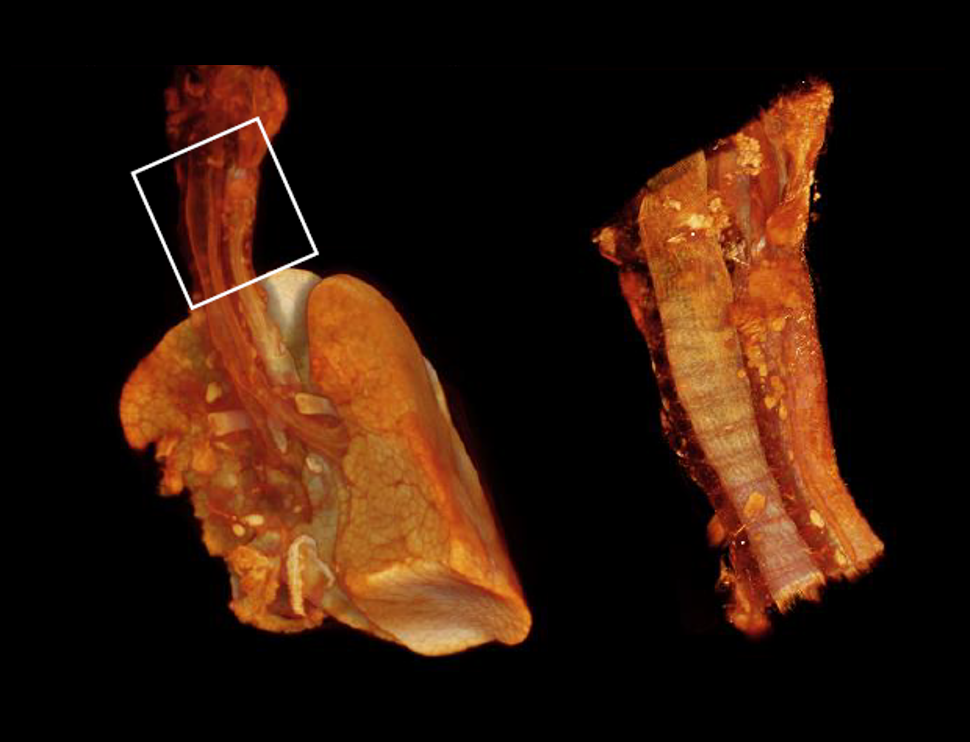
The gold standard for anatomical research is gross anatomical dissection. The main limitations for this technique are the eyes of the researcher, as structures smaller than can be perceived cannot be studied. A second look is forfeited, since visualizing some structures means excising others. An interesting alternative is scanning tissue samples by diffusible iodine-based contrast-enhanced computed tomography (diceCT), an X-ray-based method to image ex-vivo samples with microscale resolution up to 1 µm in 3D. DiceCT is progressively used in clinical and morphological research to study developmental anatomy. In collaboration with surgeons we investigate whether diceCT has additional value in studying surgical approaches.
We demonstrate the possibilities to image large stained human tissue samples in 3D with microscale resolution using diceCT. This technique bridges the gap between classical 2D histological assessment and gross anatomical dissection and guides surgeons to better understanding of the 3D microanatomy of their regions of interest. With continued advancement of dissection, staining and acquisition protocols, this method may prove invaluable for future anatomical research, education and improvement of surgical techniques.
–Daniel Docter
Embryology, diagnosis and treatment of cleft lip and palate
Palatogenesis is a complex spatiotemporal process including development and fusion of the primary and secondary palatal shelves. The complexity of this process reflects the high incidence of cleft palates in humans (~1 : 2,500 live births). In 50% of cleft palate, the cause is non-syndromic. In these cases, etiology is complicated and not yet completely understood.
Increase of embryological knowledge is crucial in adequate cleft surgery. To facilitate understanding, we are adding a 3D reconstruction of palatogenesis in different Carnegie stages in addition to the already existing ‘3D Atlas of Human Embryology’. Our cleft chapter serves both educational and clinical purposes.
Link to Palate papers: Pubmed
–Hans Smit, Prof. dr. Corstiaan Breugem
Developmental aspects of laryngeal and tracheal anomalies
My research focuses on developmental and clinical aspects of laryngeal and tracheal anomalies. These anomalies generally present in neonates with respiratory complaints like stridor, dyspnea and cyanosis, and are accountable for morbidity and mortality. The exact cause of most laryngeal and tracheal anomalies are unknown, although the development of airway cartilage seems to play an important role.
Research topics include a descriptive analysis of normal tracheal cartilage development in human embryos, an evaluation of treatment modalities for airway obstruction caused by a third or fourth branchial pouch sinus, an assessment of a new surgical technique for aortopexy in tracheobronchomalacia, and a review of tracheal anomalies in Down syndrome children.
Link to Trachea papers: Pubmed
-Matthijs Fockens, Prof. dr. Freek Dikkers
Surgical anatomy of the orbital apex
My research focusses on the anatomy of the orbital apex. We recently published a systematic review about the currently known anatomy. Now we will study the surgical anatomy of the orbital apex with a micro CT-scan. Hereafter we will study the Annulus of Zinn and it’s relationship with the optic nerve, the its precise location. After this we will look into the surgical anatomy from the supero- lateral surgical corridor to the orbital apex and skull base, using both an external approach and trans- orbital endoscopic approach. We will re-evaluate the orbital fibrous septae described by Prof. dr. Leo Koornneef and finally describe the orbital septae in the apex.
–Ozlem Engin, Prof. dr. Peerooz Saeed
